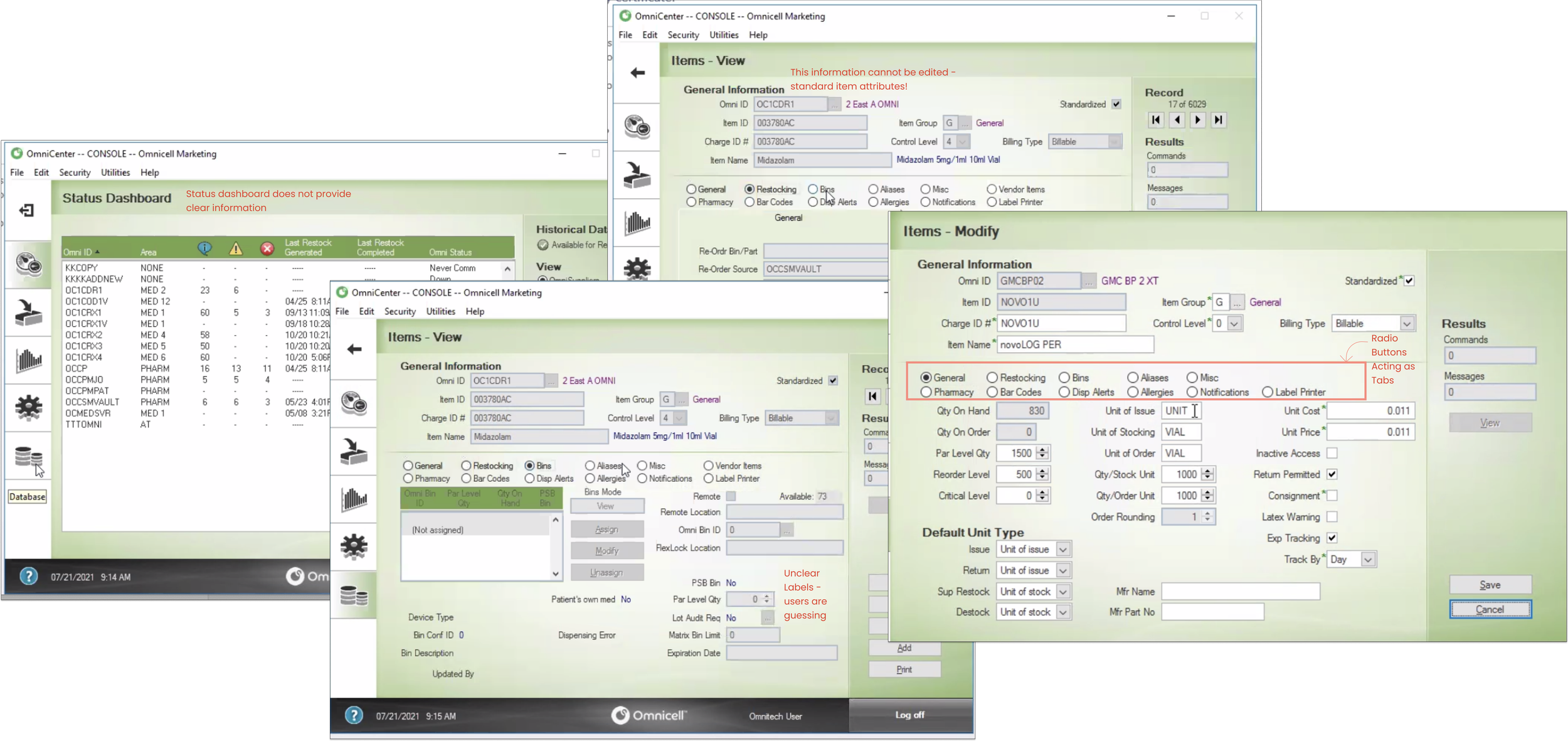
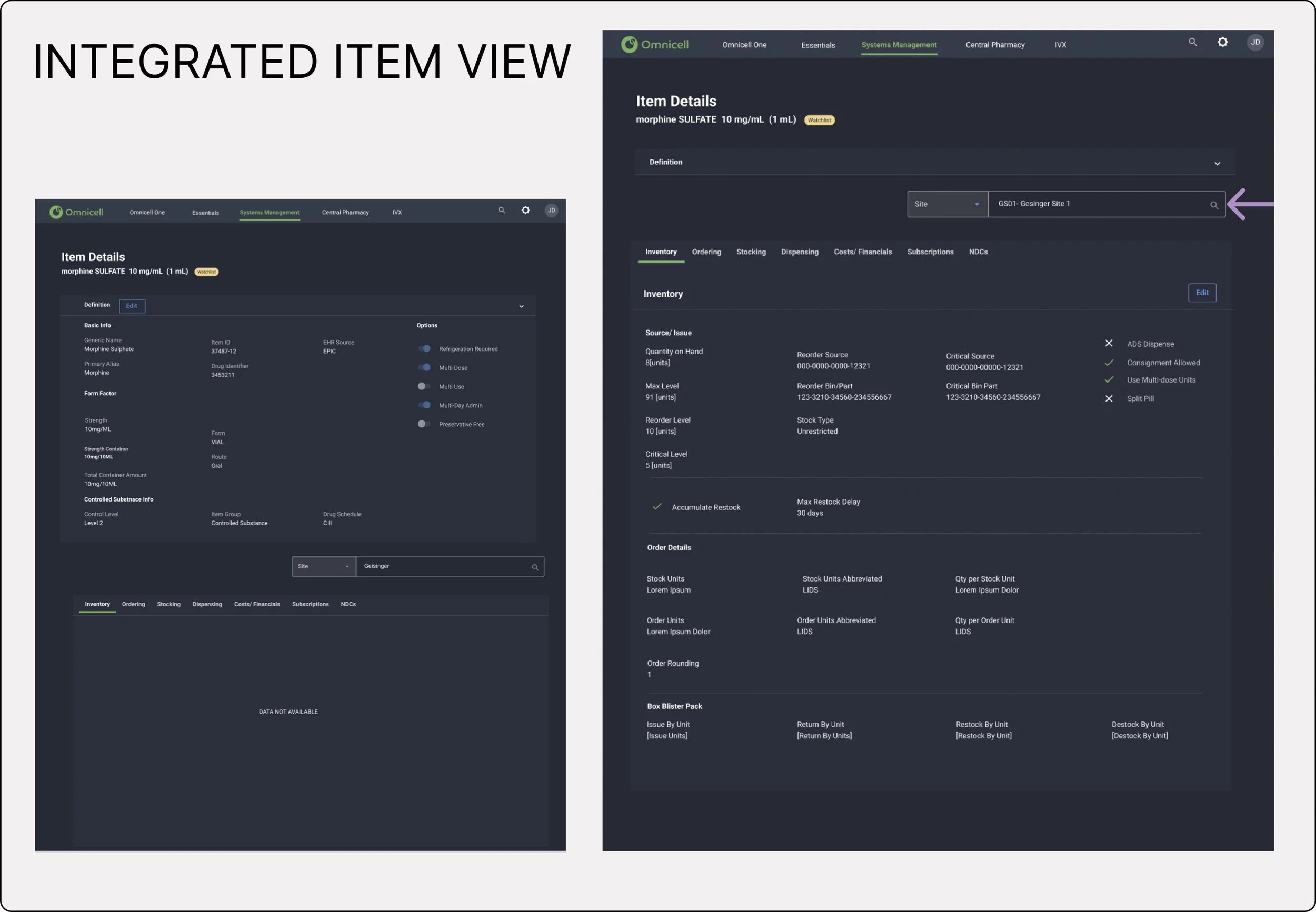
I joined Omnicell as the sole designer on the cloud platform team, facing a steep learning curve in a highly regulated, clinically complex domain. The goal: transition medication management from a legacy on-premise product to a modern cloud platform, maintaining feature parity while meaningfully improving the experience.
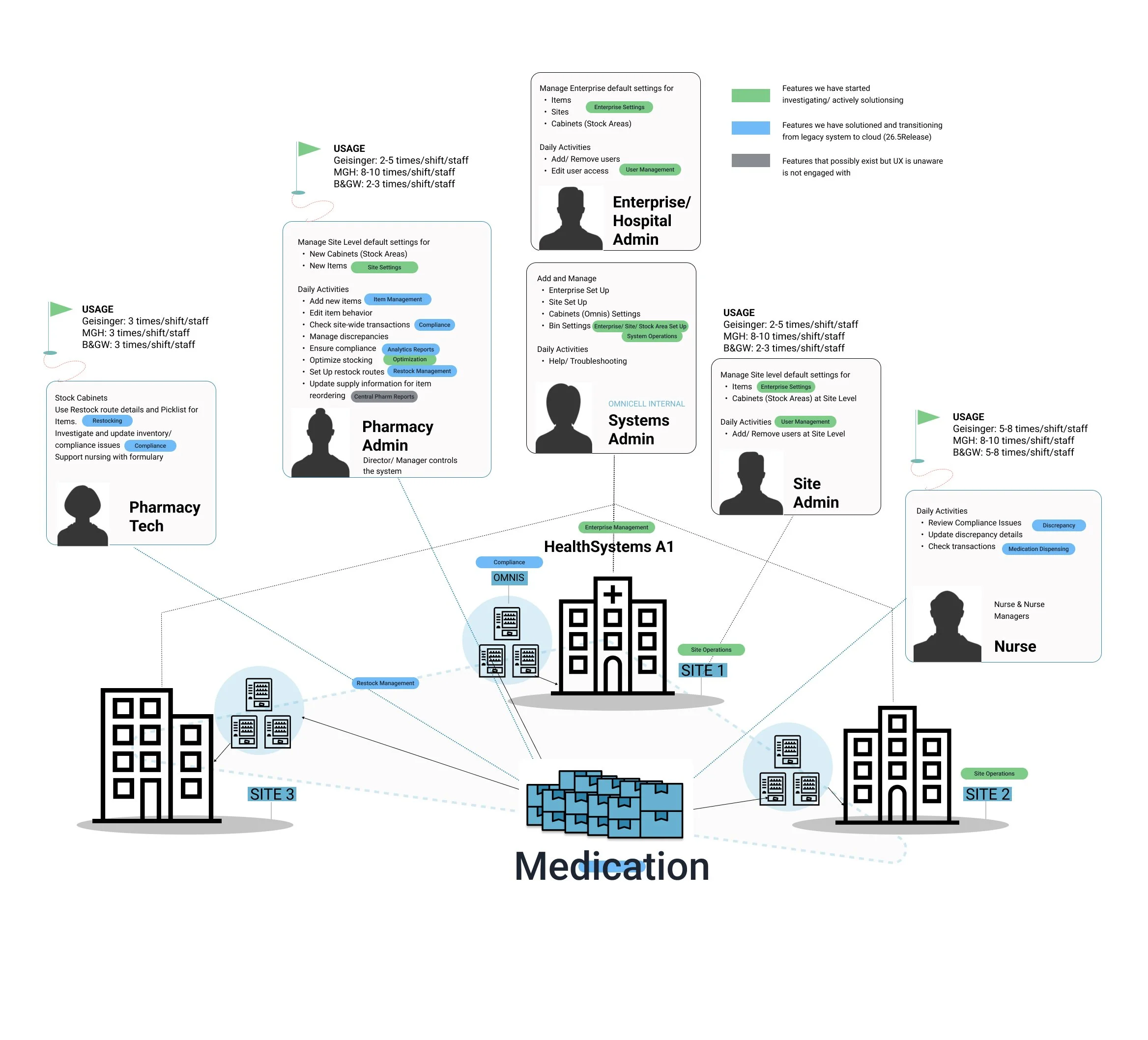
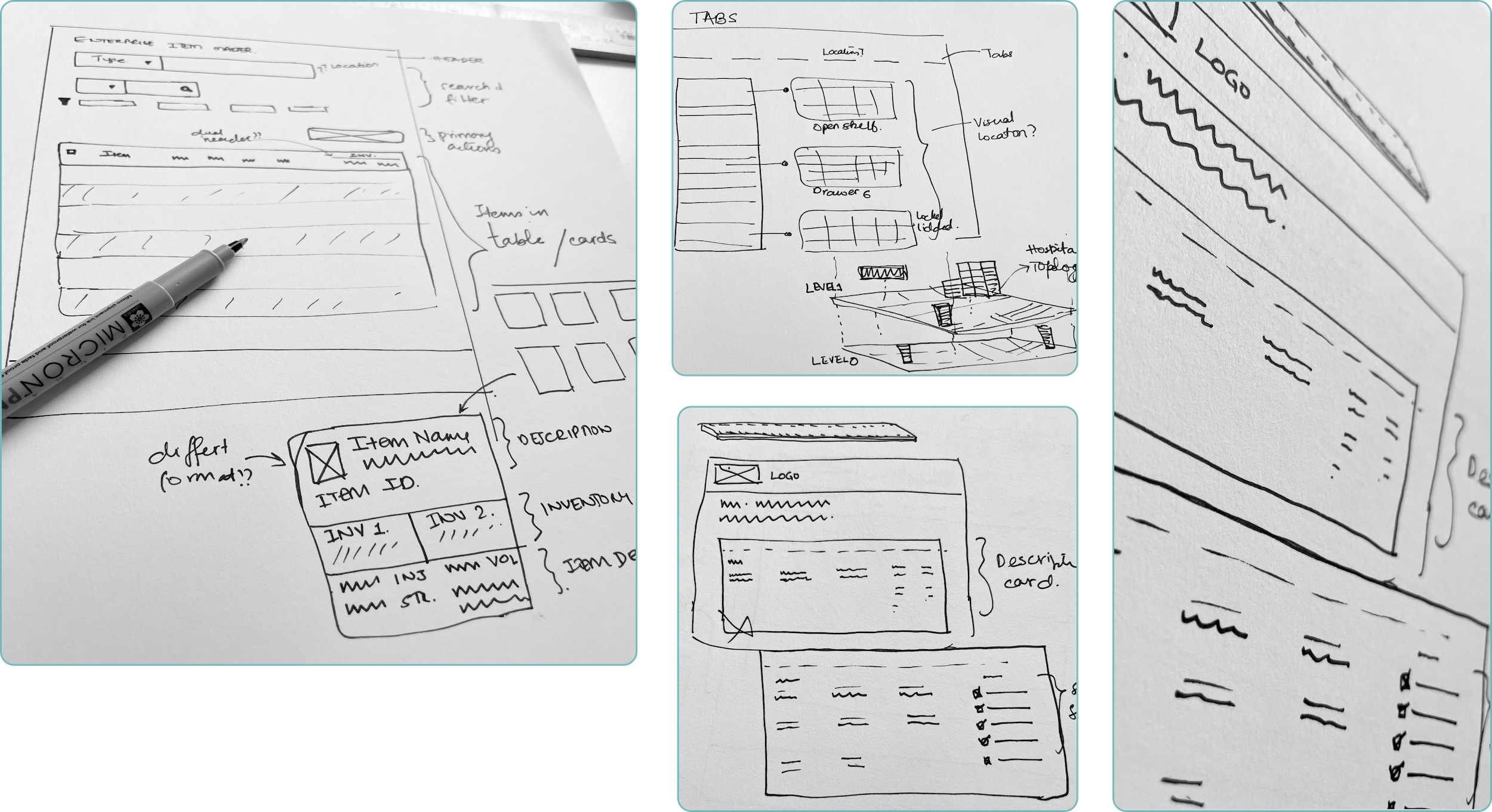
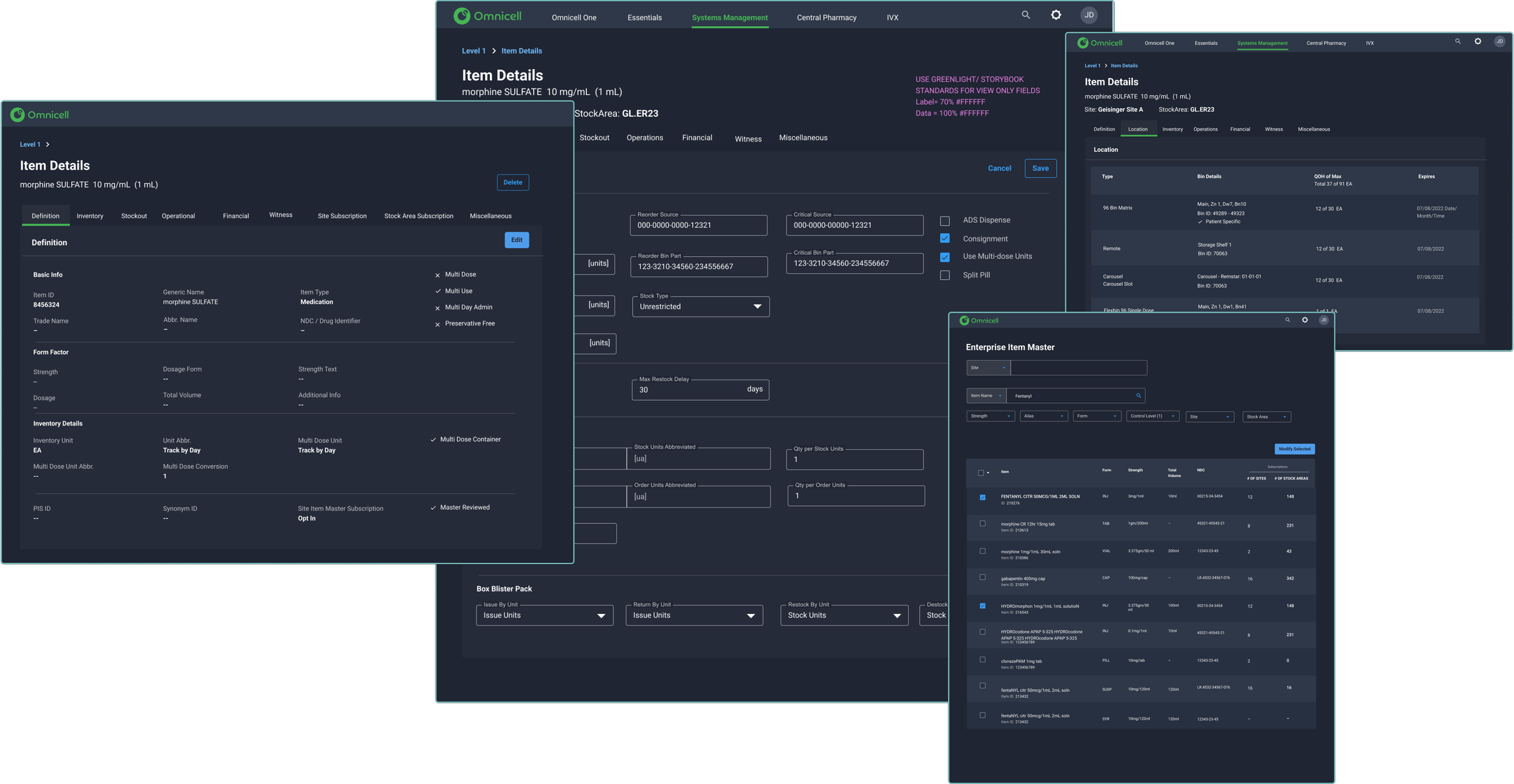
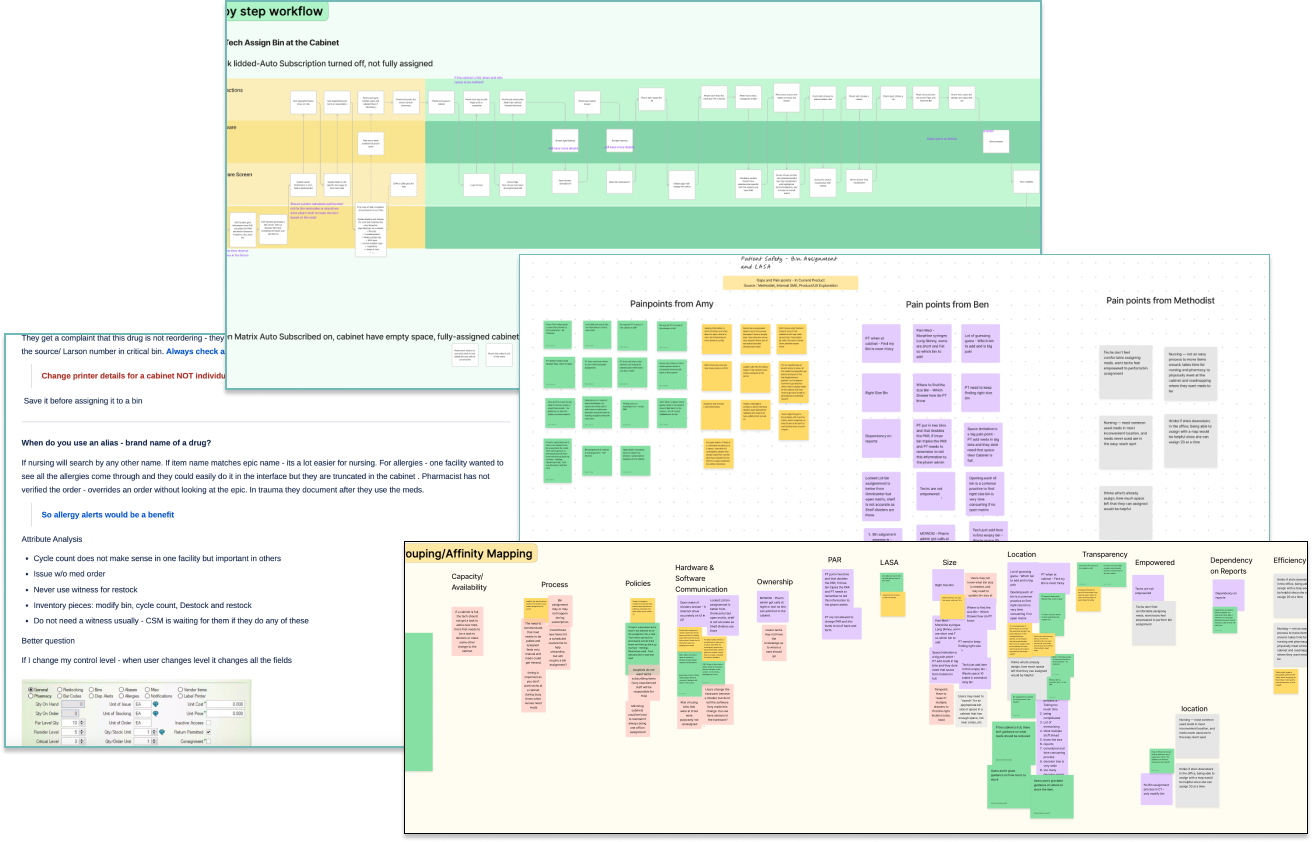
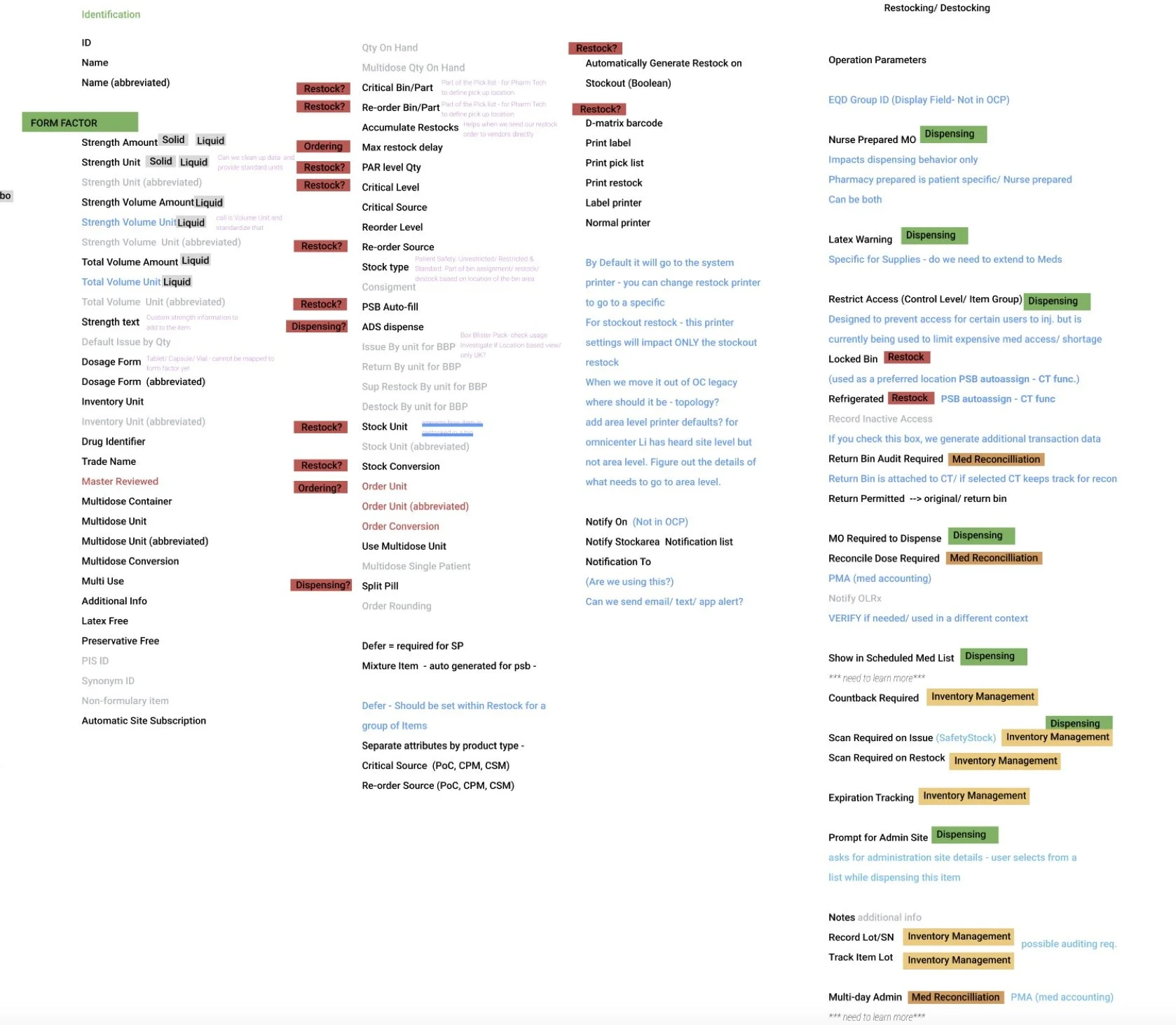
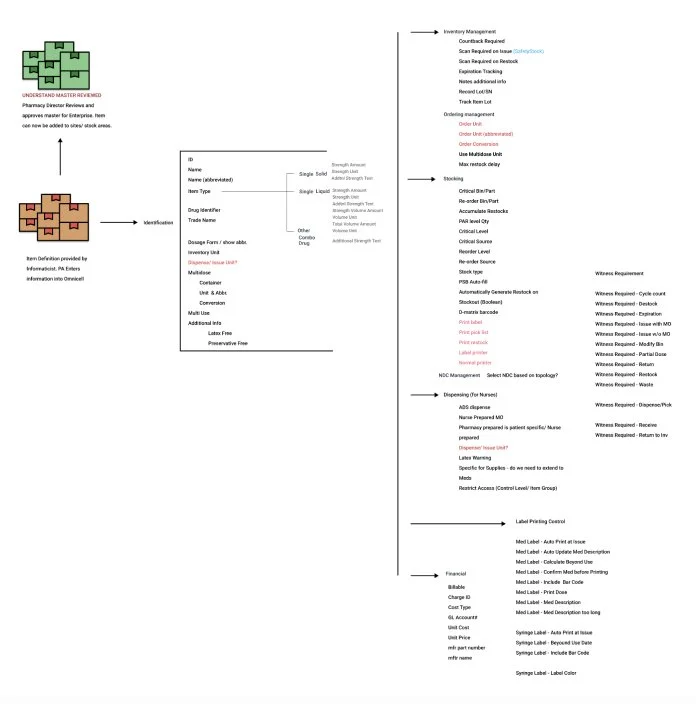
I started by establishing a design system using Material components, patterns, and icons, then delivered wireframes to unblock immediate development needs. Alongside that I conducted user studies with existing customers, collaborated with the business intelligence team on feature prioritization, and worked to align design decisions with strategic business goals.
What worked: strong engineering, product, and UX partnership, and leadership that was genuinely receptive to data and research findings.